First, pause.
You are not in immediate danger.
You do not need to decide anything today.
Your life is not ending, but it has changed.
What This Diagnosis Means and What It Does Not
Acoustic neuroma is a benign tumour. That means it is not cancer and it does not spread to other parts of the body. It does not mean it is trivial.
This tumour sits in a sensitive area near the nerves responsible for hearing and balance. That location explains why the diagnosis can feel frightening and why symptoms often seem out of proportion to what others expect.
You did not cause this.
There is usually no clear reason why it happens.
What Is Likely Happening in Your Body Right Now
Your hearing nerve and balance nerve are not working as they should. To compensate, your brain is working harder than normal just to keep you upright, oriented, and focused.
That constant effort explains many of the things you may already be experiencing:
• Hearing loss or ringing in one ear
• Dizziness or a sense of being off balance
• Fatigue that feels far heavier than normal tiredness
• Brain fog or difficulty concentrating
• Anxiety that feels physical, not just emotional
These symptoms are real. They are neurological. You are not imagining them.
What You Need to Know Today
Not Everything
You do not need to make treatment decisions right now.
Many people are safely monitored for months or even years before any intervention is needed.
Growth is usually slow. One MRI scan does not tell the full story. Clarity comes from time and repeat scans, not from urgency or panic.
Symptoms and tumour size do not always match. Feeling unwell does not automatically mean the tumour is growing quickly.
If treatment becomes necessary, recovery is often longer than doctors initially suggest. That is not because something has gone wrong. It is because the brain heals slowly.
About Hearing and Balance
Some hearing loss with acoustic neuroma is permanent. In some people it stabilises. In others it worsens. There is no reliable way to predict which path you will follow.
Balance issues and dizziness are common. Your brain can adapt, but this adaptation takes time and energy.
Fatigue and brain fog are part of this condition. They are not signs of weakness, laziness, or psychological failure.
About Fear, Shock, and Mental Overload
Feeling frightened does not mean you are coping badly. It means you understand that this diagnosis matters.
The word benign often confuses people around you. Some may minimise what you are going through because they hear “not cancer.” That can be deeply invalidating. It does not mean they are right.
You do not owe anyone a detailed explanation. Especially not right now.
What You Should Not Do in the Early Days
Do not rush into treatment decisions.
Do not compare yourself to other patients online.
Do not assume the worst case applies to you.
Do not expect yourself to function normally.
Your nervous system is under strain. Give it space.
What Helps in the First Few Days
Write your questions down. Memory and focus are often unreliable at this stage.
Bring someone you trust to medical appointments.
Limit how much information you consume in one sitting.
Rest more than you think you should.
If your body asks for rest, listen to it.
What This Diagnosis Does Not Take Away
Your intelligence.
Your value.
Your ability to live a meaningful life.
Many people with acoustic neuroma continue to work, love, travel, adapt, and rebuild full lives. Often differently. Often more slowly. Still fully.
One Last Thing to Hold On To
You are allowed to grieve the version of life you thought you had.
You are also allowed to take this one day at a time.
Today is about stabilising, not solving.
Tomorrow can wait.
If this post helped you feel less lost, share it with others who may be sitting in the same uncertainty.
Wishing you a peaceful Christmas from my family to yours.
Amir
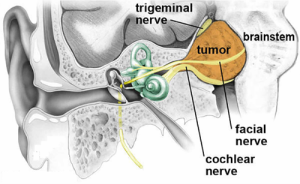 The fourth nerve passing through the canal is the facial nerve which supplies movements of the face and very rarely a Schwannoma can affect this nerve. This is known as a facial neuroma.
The fourth nerve passing through the canal is the facial nerve which supplies movements of the face and very rarely a Schwannoma can affect this nerve. This is known as a facial neuroma.